MHA
MHA Active Companion - Health advices that remember you
Year
2026
Category
AI Personalisation · Digital Health
Client
Musculoskeletal Health Australia
/ Problem
Trusted Information in the Age of Instant Answers
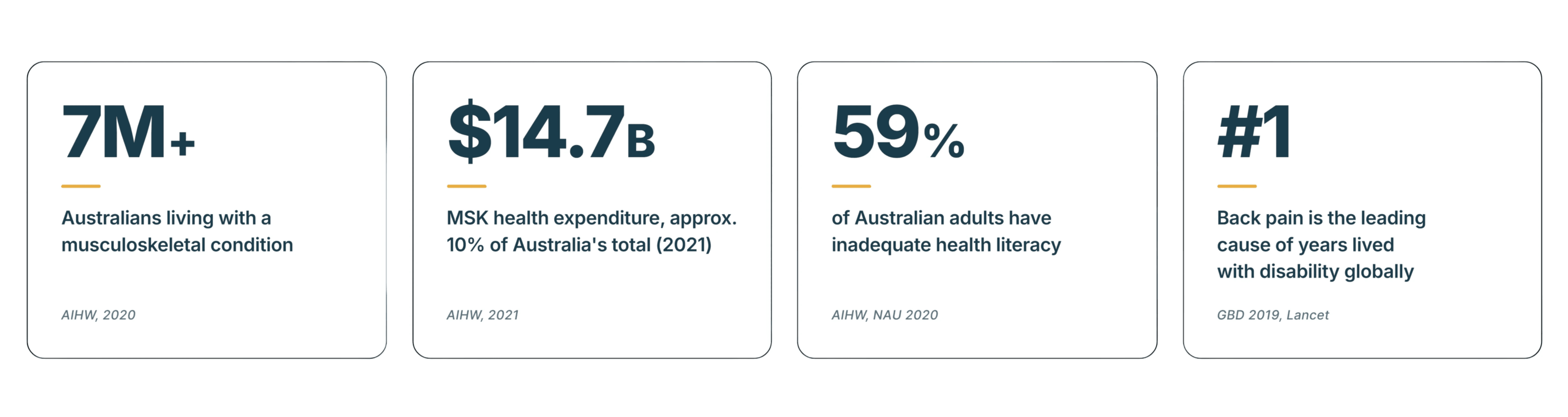
Musculoskeletal Health Australia serves the 7.3 million Australians affected by musculoskeletal conditions through clinically vetted health information and a national helpline. Generative AI has made health answers instant and free, and the knowledge-based value MHA spent fifty years building is harder to differentiate on access alone.
The strategy is moving from purely providing health knowledge to actively personalising and guiding its execution.
Information overload, fragmented content, no user profiling, single-visit disengagement - reduced to one root cause: the failure of continuous engagement. MHA provides health information but doesn't have a structured pathway to convert it into sustained behaviour change. That diagnosis also defines what a chatbot cannot replicate - information accountability and a relationship that persists, a companion that knows the user's risk, tracks their progress, and adapts as their condition changes. The strategy moves MHA's value from owning answers to maintaining that relationship.
/ Product Pathway
Assess on the Website, Sustain in the App
The solution has two integrated parts. A website-based risk assessment delivers complete value with no app download: a 13-question, clinically approved questionnaire, one per screen, scored by a deterministic rule-based engine into Low, Medium, or High risk.
A companion app converts that one-time result into ongoing support through check-ins, adaptive nudges, goal tailoring, and reassessment: an engagement design mapped onto the Fogg Behaviour Model's motivation–ability–prompt structure.

/ Features
What Was Delivered
Three months of research and design produced a solid product plan: resolved flows, mapped architecture, scoped priorities and phases, everything engineering needs to estimate accurately and build without guesswork.

Scoring by Rules, AI Confined to Language
The architecture separates deterministic clinical logic from generative AI. A large language model, constrained to MHA's approved content library, generates the personalised action plan and rewrites it at Grade 7-8 readability - usable guidance for the 59% of Australian adults with inadequate health literacy. The app uses only what users deliberately enter, keeping the risk result explainable and the data practice compliant with the Australian Privacy Principles, no behavioural tracking, no location data, no time-in-app measurement.

Personalisation at Two Levels
The risk tier determines the type of support:
Low: Prevention at Low
Medium: Active behaviour change
High: Clinical Routing at High
MHA's B.A.M. helpline first and GP referral second. Individual context then determines the plan's shape: a construction worker and an office worker at the same Medium tier receive different plans, safe-lifting technique and post-shift recovery for one, posture resets, and movement breaks for the other. All personalisation runs on data are captured in the assessment.

Check-ins That Serve as Memory
Check-ins are how the system remembers and responds. Questions stay fixed within each tier; consistency is what makes pattern detection possible, while frequency and depth are calibrated to risk.
Low risk: two questions biweekly, checking early signs of escalation
Medium: three weekly, combining habit adherence with pain tracking to separate disengaged users from engaged ones who need plan adjustments
High: four weekly, pain first, with "It was too painful" available as an adherence answer, recording non-completion as a symptom.

Two design details support the loop:
The Stretch function bundles exercise choice, sequencing, and timing into a single tap, a guided two-minute desk reset with on-screen cues and a built-in timer, logged automatically, removing the friction between intending a movement and doing it.
At High risk: A "struggling" response on the mood check conditionally surfaces mental-health support (Beyond Blue, Lifeline) as the dashboard's top item, presents when needed.

Reassessment That Moves Both Ways
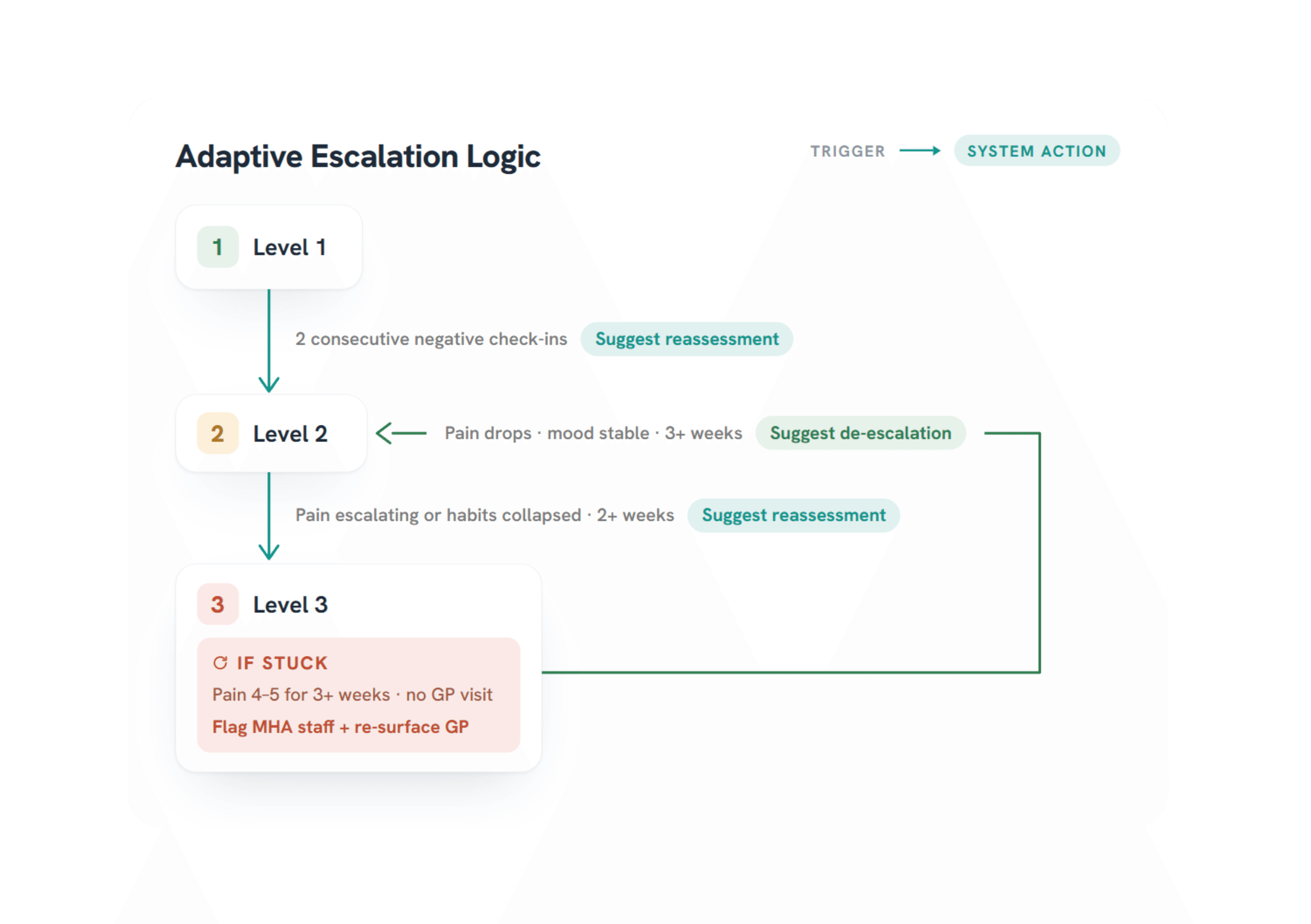
Users can retake the assessment at any time, with no cooldowns or prerequisites. The system also suggests reassessment when check-in patterns warrant it. Triggers run in both directions: sustained decline surfaces a reassessment prompt, while three stable weeks at High risk surface the option to move down a tier. Assessment history is retained so users can track their trajectory.

Staying With the User Into Clinical Care
One positioning tension had to be resolved: emphasising GP referral risked contradicting MHA's preventative mission.
The resolution was positioning as MHA staying with the user into clinical care: preventative before a condition emerges, and preventative of it worsening.
The Tailor Hub carries this through. Users set their own goals alongside the generated plan, and can upload advice from their physiotherapist or GP, converted into trackable goals through tag-based categorisation rather than AI interpretation of clinical notes. MHA does not compete with the clinician; it becomes what makes clinical advice actionable and tracked over time.

Notifications That Know When to Stop
The notification strategy balances two legitimate needs: the client's need to keep users engaged and the user's control over their own attention. Active users receive contextual nudges shaped by their questionnaire data - tied to work rhythm for an office worker, to shift patterns for a construction worker, with user-set frequency, timing, and tone.
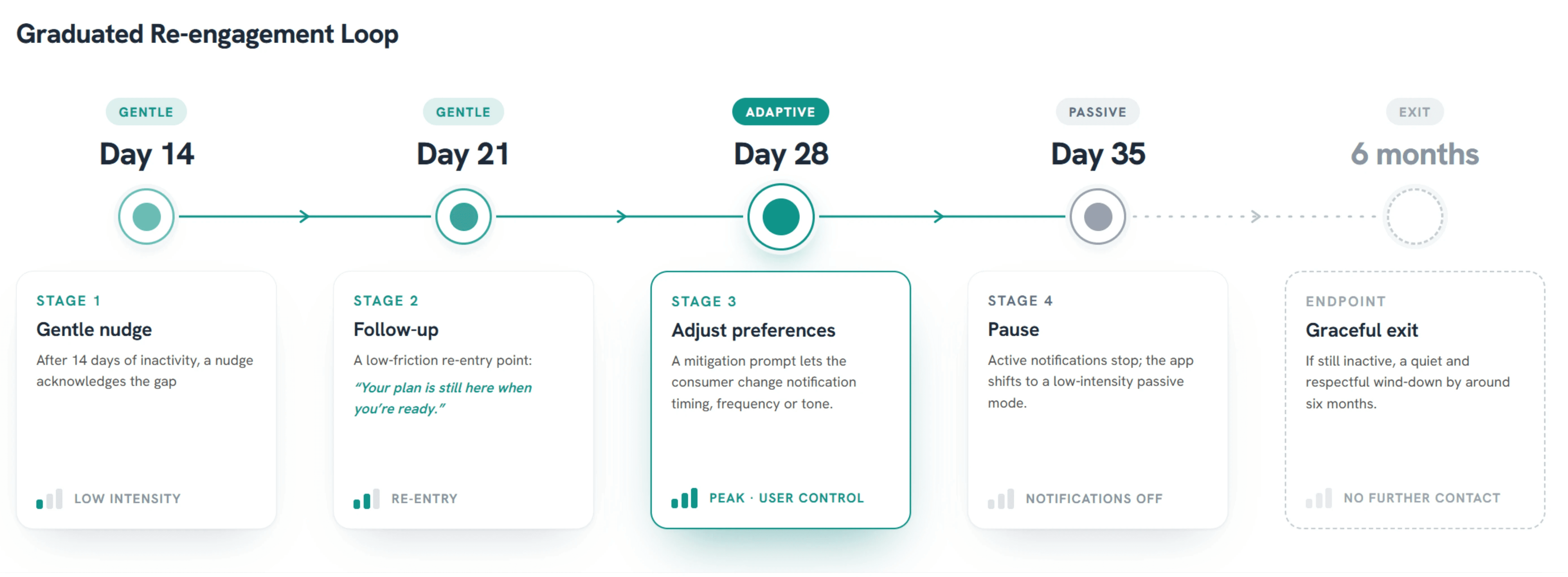
Re-engagement after inactivity is graduated: a nudge at 14 days, a low-friction re-entry at 21, a preference adjustment at 28, and a stand-down to passive mode at 35. After six months, a graceful exit with full data control: pause, delete, or return later.

The Loop MHA Can See
Continuous engagement also requires organisational visibility; MHA can only sustain a loop it can see. A staff dashboard tracks engagement rates, check-in completion, and active care journeys, segments users by support demand, and flags sustained low engagement or reported physical and mental-health concerns for proactive outreach, closing the engagement loop on the organisation's side.
An Implementation MHA Can Fund
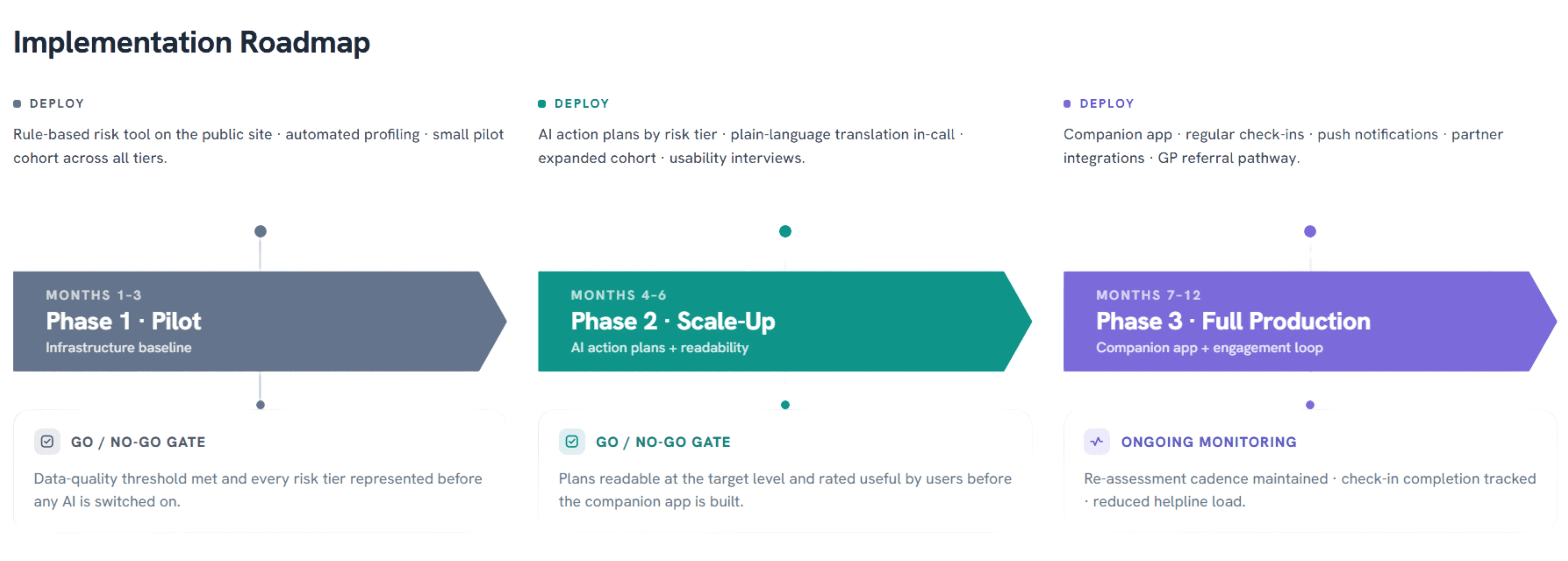
The rollout phases across twelve months: website pilot, AI layer, then companion app, and each phase must earn the next through defined go/no-go gates: data reliability before any AI is deployed, validated readability and plan usefulness before the app is built, and in production, diverting 40% of low- and medium-risk helpline contacts to self-management so staff time concentrates on the calls that need a human.
The build was costed in full and engineered to fit the budget: MHA's existing CRM/identity layer, an off-the-shelf LLM via API, and a complete design package: interactive prototype, information architecture, and engineering handoff, reducing time for integration. The platform is condition-agnostic (extending to osteoarthritis or gout is new content, not a new build), and the staff dashboard doubles as the evidence base for MHA's funding applications.
The deliverable is a build-ready strategy with a working prototype.
/ What This Work Demonstrates
The work answers a question that many content organisations now face: when AI makes information free, value moves to the relationship. The system demonstrates that shift end-to-end, AI placed where it adds capability (language, personalisation), kept out of where it erodes trust (scoring, diagnosis), and packaged so the client could realistically fund it.
MHA
MHA Active Companion - Health advices that remember you
Year
2026
Category
AI Personalisation · Digital Health
Client
Musculoskeletal Health Australia
/ Problem
Trusted Information in the Age of Instant Answers
Musculoskeletal Health Australia serves the 7.3 million Australians affected by musculoskeletal conditions through clinically vetted health information and a national helpline. Generative AI has made health answers instant and free, and the knowledge-based value MHA spent fifty years building is harder to differentiate on access alone.
The strategy is moving from purely providing health knowledge to actively personalising and guiding its execution.
Information overload, fragmented content, no user profiling, single-visit disengagement - reduced to one root cause: the failure of continuous engagement. MHA provides health information but doesn't have a structured pathway to convert it into sustained behaviour change. That diagnosis also defines what a chatbot cannot replicate - information accountability and a relationship that persists, a companion that knows the user's risk, tracks their progress, and adapts as their condition changes. The strategy moves MHA's value from owning answers to maintaining that relationship.
/ Product Pathway
Assess on the Website, Sustain in the App
The solution has two integrated parts. A website-based risk assessment delivers complete value with no app download: a 13-question, clinically approved questionnaire, one per screen, scored by a deterministic rule-based engine into Low, Medium, or High risk.
A companion app converts that one-time result into ongoing support through check-ins, adaptive nudges, goal tailoring, and reassessment: an engagement design mapped onto the Fogg Behaviour Model's motivation–ability–prompt structure.
/ Features
What Was Delivered
Three months of research and design produced a solid product plan: resolved flows, mapped architecture, scoped priorities and phases, everything engineering needs to estimate accurately and build without guesswork.
Scoring by Rules, AI Confined to Language
The architecture separates deterministic clinical logic from generative AI. A large language model, constrained to MHA's approved content library, generates the personalised action plan and rewrites it at Grade 7-8 readability - usable guidance for the 59% of Australian adults with inadequate health literacy. The app uses only what users deliberately enter, keeping the risk result explainable and the data practice compliant with the Australian Privacy Principles, no behavioural tracking, no location data, no time-in-app measurement.
Personalisation at Two Levels
The risk tier determines the type of support:
Low: Prevention at Low
Medium: Active behaviour change
High: Clinical Routing at High
MHA's B.A.M. helpline first and GP referral second. Individual context then determines the plan's shape: a construction worker and an office worker at the same Medium tier receive different plans, safe-lifting technique and post-shift recovery for one, posture resets, and movement breaks for the other. All personalisation runs on data are captured in the assessment.
Check-ins That Serve as Memory
Check-ins are how the system remembers and responds. Questions stay fixed within each tier; consistency is what makes pattern detection possible, while frequency and depth are calibrated to risk.
Low risk: two questions biweekly, checking early signs of escalation
Medium: three weekly, combining habit adherence with pain tracking to separate disengaged users from engaged ones who need plan adjustments
High: four weekly, pain first, with "It was too painful" available as an adherence answer, recording non-completion as a symptom.
Two design details support the loop:
The Stretch function bundles exercise choice, sequencing, and timing into a single tap, a guided two-minute desk reset with on-screen cues and a built-in timer, logged automatically, removing the friction between intending a movement and doing it.
At High risk: A "struggling" response on the mood check conditionally surfaces mental-health support (Beyond Blue, Lifeline) as the dashboard's top item, presents when needed.
Reassessment That Moves Both Ways
Users can retake the assessment at any time, with no cooldowns or prerequisites. The system also suggests reassessment when check-in patterns warrant it. Triggers run in both directions: sustained decline surfaces a reassessment prompt, while three stable weeks at High risk surface the option to move down a tier. Assessment history is retained so users can track their trajectory.
Staying With the User Into Clinical Care
One positioning tension had to be resolved: emphasising GP referral risked contradicting MHA's preventative mission.
The resolution was positioning as MHA staying with the user into clinical care: preventative before a condition emerges, and preventative of it worsening.
The Tailor Hub carries this through. Users set their own goals alongside the generated plan, and can upload advice from their physiotherapist or GP, converted into trackable goals through tag-based categorisation rather than AI interpretation of clinical notes. MHA does not compete with the clinician; it becomes what makes clinical advice actionable and tracked over time.
Notifications That Know When to Stop
The notification strategy balances two legitimate needs: the client's need to keep users engaged and the user's control over their own attention. Active users receive contextual nudges shaped by their questionnaire data - tied to work rhythm for an office worker, to shift patterns for a construction worker, with user-set frequency, timing, and tone.
Re-engagement after inactivity is graduated: a nudge at 14 days, a low-friction re-entry at 21, a preference adjustment at 28, and a stand-down to passive mode at 35. After six months, a graceful exit with full data control: pause, delete, or return later.
The Loop MHA Can See
Continuous engagement also requires organisational visibility; MHA can only sustain a loop it can see. A staff dashboard tracks engagement rates, check-in completion, and active care journeys, segments users by support demand, and flags sustained low engagement or reported physical and mental-health concerns for proactive outreach, closing the engagement loop on the organisation's side.
An Implementation MHA Can Fund
The rollout phases across twelve months: website pilot, AI layer, then companion app, and each phase must earn the next through defined go/no-go gates: data reliability before any AI is deployed, validated readability and plan usefulness before the app is built, and in production, diverting 40% of low- and medium-risk helpline contacts to self-management so staff time concentrates on the calls that need a human.
The build was costed in full and engineered to fit the budget: MHA's existing CRM/identity layer, an off-the-shelf LLM via API, and a complete design package: interactive prototype, information architecture, and engineering handoff, reducing time for integration. The platform is condition-agnostic (extending to osteoarthritis or gout is new content, not a new build), and the staff dashboard doubles as the evidence base for MHA's funding applications.
The deliverable is a build-ready strategy with a working prototype.
/ What This Work Demonstrates
The work answers a question that many content organisations now face: when AI makes information free, value moves to the relationship. The system demonstrates that shift end-to-end, AI placed where it adds capability (language, personalisation), kept out of where it erodes trust (scoring, diagnosis), and packaged so the client could realistically fund it.
MHA
MHA Active Companion - Health advices that remember you
Year
2026
Category
AI Personalisation · Digital Health
Client
Musculoskeletal Health Australia
/ Problem
Trusted Information in the Age of Instant Answers
Musculoskeletal Health Australia serves the 7.3 million Australians affected by musculoskeletal conditions through clinically vetted health information and a national helpline. Generative AI has made health answers instant and free, and the knowledge-based value MHA spent fifty years building is harder to differentiate on access alone.
The strategy is moving from purely providing health knowledge to actively personalising and guiding its execution.
Information overload, fragmented content, no user profiling, single-visit disengagement - reduced to one root cause: the failure of continuous engagement. MHA provides health information but doesn't have a structured pathway to convert it into sustained behaviour change. That diagnosis also defines what a chatbot cannot replicate - information accountability and a relationship that persists, a companion that knows the user's risk, tracks their progress, and adapts as their condition changes. The strategy moves MHA's value from owning answers to maintaining that relationship.
/ Product Pathway
Assess on the Website, Sustain in the App
The solution has two integrated parts. A website-based risk assessment delivers complete value with no app download: a 13-question, clinically approved questionnaire, one per screen, scored by a deterministic rule-based engine into Low, Medium, or High risk.
A companion app converts that one-time result into ongoing support through check-ins, adaptive nudges, goal tailoring, and reassessment: an engagement design mapped onto the Fogg Behaviour Model's motivation–ability–prompt structure.
/ Features
What Was Delivered
Three months of research and design produced a solid product plan: resolved flows, mapped architecture, scoped priorities and phases, everything engineering needs to estimate accurately and build without guesswork.
Scoring by Rules, AI Confined to Language
The architecture separates deterministic clinical logic from generative AI. A large language model, constrained to MHA's approved content library, generates the personalised action plan and rewrites it at Grade 7-8 readability - usable guidance for the 59% of Australian adults with inadequate health literacy. The app uses only what users deliberately enter, keeping the risk result explainable and the data practice compliant with the Australian Privacy Principles, no behavioural tracking, no location data, no time-in-app measurement.
Personalisation at Two Levels
The risk tier determines the type of support:
Low: Prevention at Low
Medium: Active behaviour change
High: Clinical Routing at High
MHA's B.A.M. helpline first and GP referral second. Individual context then determines the plan's shape: a construction worker and an office worker at the same Medium tier receive different plans, safe-lifting technique and post-shift recovery for one, posture resets, and movement breaks for the other. All personalisation runs on data are captured in the assessment.
Check-ins That Serve as Memory
Check-ins are how the system remembers and responds. Questions stay fixed within each tier; consistency is what makes pattern detection possible, while frequency and depth are calibrated to risk.
Low risk: two questions biweekly, checking early signs of escalation
Medium: three weekly, combining habit adherence with pain tracking to separate disengaged users from engaged ones who need plan adjustments
High: four weekly, pain first, with "It was too painful" available as an adherence answer, recording non-completion as a symptom.
Two design details support the loop:
The Stretch function bundles exercise choice, sequencing, and timing into a single tap, a guided two-minute desk reset with on-screen cues and a built-in timer, logged automatically, removing the friction between intending a movement and doing it.
At High risk: A "struggling" response on the mood check conditionally surfaces mental-health support (Beyond Blue, Lifeline) as the dashboard's top item, presents when needed.
Reassessment That Moves Both Ways
Users can retake the assessment at any time, with no cooldowns or prerequisites. The system also suggests reassessment when check-in patterns warrant it. Triggers run in both directions: sustained decline surfaces a reassessment prompt, while three stable weeks at High risk surface the option to move down a tier. Assessment history is retained so users can track their trajectory.
Staying With the User Into Clinical Care
One positioning tension had to be resolved: emphasising GP referral risked contradicting MHA's preventative mission.
The resolution was positioning as MHA staying with the user into clinical care: preventative before a condition emerges, and preventative of it worsening.
The Tailor Hub carries this through. Users set their own goals alongside the generated plan, and can upload advice from their physiotherapist or GP, converted into trackable goals through tag-based categorisation rather than AI interpretation of clinical notes. MHA does not compete with the clinician; it becomes what makes clinical advice actionable and tracked over time.
Notifications That Know When to Stop
The notification strategy balances two legitimate needs: the client's need to keep users engaged and the user's control over their own attention. Active users receive contextual nudges shaped by their questionnaire data - tied to work rhythm for an office worker, to shift patterns for a construction worker, with user-set frequency, timing, and tone.
Re-engagement after inactivity is graduated: a nudge at 14 days, a low-friction re-entry at 21, a preference adjustment at 28, and a stand-down to passive mode at 35. After six months, a graceful exit with full data control: pause, delete, or return later.
The Loop MHA Can See
Continuous engagement also requires organisational visibility; MHA can only sustain a loop it can see. A staff dashboard tracks engagement rates, check-in completion, and active care journeys, segments users by support demand, and flags sustained low engagement or reported physical and mental-health concerns for proactive outreach, closing the engagement loop on the organisation's side.
An Implementation MHA Can Fund
The rollout phases across twelve months: website pilot, AI layer, then companion app, and each phase must earn the next through defined go/no-go gates: data reliability before any AI is deployed, validated readability and plan usefulness before the app is built, and in production, diverting 40% of low- and medium-risk helpline contacts to self-management so staff time concentrates on the calls that need a human.
The build was costed in full and engineered to fit the budget: MHA's existing CRM/identity layer, an off-the-shelf LLM via API, and a complete design package: interactive prototype, information architecture, and engineering handoff, reducing time for integration. The platform is condition-agnostic (extending to osteoarthritis or gout is new content, not a new build), and the staff dashboard doubles as the evidence base for MHA's funding applications.
The deliverable is a build-ready strategy with a working prototype.
/ What This Work Demonstrates
The work answers a question that many content organisations now face: when AI makes information free, value moves to the relationship. The system demonstrates that shift end-to-end, AI placed where it adds capability (language, personalisation), kept out of where it erodes trust (scoring, diagnosis), and packaged so the client could realistically fund it.